Comprehensive management of unilateral cleft lip and palate patient-a - A Case report
Anjumanpreet Kaur Dua M.D.S ,Associate professor , Dept. of Orthodontics and Dentofacial Orthopaedics, Baba Jaswant Singh Dental College, Ludhiana , Punjab , India.
Ajit Kumar Jaiswal M.D.S, Associate professor ,Dept. of Orthodontics and Dentofacial Orthopaedics, Christian Dental College, C.M.C, Ludhiana , Punjab India.
Laxman Kumar Rangnathan M.D.S Associate professor ,Dept. of Oral& Maxillofacial surgery, Christian Dental College, C.M.C, Ludhiana , Punjab , India.
Kavitha Eppen. Assistant professor, Dept. of Orthodontics and Dentofacial Orthopaedics Christian Dental College, C.M.C Ludhiana , Punjab India.
Praveen Kumar Neela M.D.S, Assistant professor ,Dept. of Orthodontics and Dentofacial Orthopaedics , Kamineni Institute of Dental Sciences, Narkatpally, Andhra Pradesh, India.
Corresponding Author-
Dr. Ajit Kumar Jaiswal M.D.S, Associate professor ,Dept. of Orthodontics and Dentofacial Orthopaedics, Christian Dental College,C.M.C, Ludhiana , Punjab India.
E-mail- [email protected]
Contact no-91-9876445320
Para efectos de referencia bibliográfica este trabajo debe ser citado de la siguiente manera:
Anjumanpreet Kaur Dua., Ajit Kumar Jaiswal., Laxman Kumar Rangnathan ., Kavitha Eppen., Praveen Kumar Neela ." COMPREHENSIVE MANAGEMENT OF UNILATERAL CLEFT LIP AND PALATE PATIENT-A - A CASE REPORT ."
Revista Latinoamericana de Ortodoncia y Odontopediatría "Ortodoncia.ws edición electrónica Marzo 2012. Obtenible en: www.ortodoncia.ws. Consultada, / /
RESUMEN: Introducción. Paladar y labio leporino son una malformación congénita común. Estos pacientes tienen multitud de problemas como la desfiguración facial, fonación indebida, regurgitación nasal y varios dientes de faltantes. El cierre óseo de la hendidura alveolar que se requiere para la formación de regular arco dental superior, ocupa una posición especial con en el concepto de la terapia de labio y paladar hendido. Examen e historia clínica. Una paciente 17 años de edad con labio y paladar hendido unilateral referida para tratamiento. Presentó un patrón mesofacial, perfil ortognático, mentón ligeramente prominente con el tabique nasal desviado hacia la derecha. Examen intra oral reveló que tenía el proceso alveolar hendido. Tenía valores cefalométricos de maloclusión clase I con mordida Cruzada y varios dientes perdidos. Tratamiento y resultados. La paciente había sido tratada con dispositivo de Roth.018 junto con plano de mordida anterior para la corrección de mordida Cruzada durante 16 meses. Tras 8 meses de alineación, fue hecho el injerto de hueso alveolar. 2 años post tratamiento el registro muestra que los resultados del tratamiento fueron estables, pero el IPOA reveló que el injerto de hueso alveolar se absorbe en ausencia de estímulo funcional. Discusión. Se ha demostrado que cuando la hendidura alveolar está cubierta por el puente, el hueso injertado sufre una reabsorción mayor debido a la falta de estrés funcional. El presente caso sirve para reforzar que clínico debe mover dientes adyacentes al hueso injertado o motivar al paciente para usar una prótesis de implante apoyado a fin de proporcionar estímulo funcional para el éxito de injerto de hueso alveolar.
ABSTRACT Introduction. Cleft lip and palate is a common congenital malformation. These patients have multitude of problems like facial disfigurement, improper speech, nasal regurgitation and several missing and malformed teeth. The osseous closure of the alveolar cleft, which is required for the formation of regular upper dental arch, occupies a special position with in the whole concept of cleft lip and palate therapy. History and Clinical examination. A 17 year old female patient with unilateral cleft lip and palate reported to us for treatment. She presented a mesoprosopic facial pattern, orthognathic profile, slightly prominent chin with deviated nasal septum towards right side. Intra oral examination revealed that she also had alveolar cleft. She had Angles Class I malocclusion with cross bite and several missing teeth. Treatment and Results. She had been treated with .018 Roth appliance in conjunction with anterior bite plane for correction of cross bite for 16 months. After 8 months of arch alignment alveolar bone grafting was done. 2 years post treatment record shows that treatment results were stable, but serial IOPA revealed that alveolar bone graft was resorbed in absence of functional stimulus. Discussion. It has been shown that when alveolar cleft is covered by bridge, grafted bone undergoes a greater resorption due to missing functional stress. The present case reinforce that clinician should move adjacent teeth in to the grafted bone or motivate the patient for implant supported prosthesis in order to provide functional stimulus for the success for alveolar bone graft.
INTRODUCTION
Cleft lip and palate is a common congenital malformation. These patients have multitude of problems like facial disfigurement, improper speech, nasal regurgitation and several missing and malformed teeth .These are the patients who requires special care. The incidence for morphologic irregularities is higher for all teeth. In those patient, a congenitally missing permanent maxillary lateral incisor on the cleft site is the most common finding (1, 2). The successful treatment of patients with complete clefts of lip, palate and alveolus requires a continuous interdisciplinary therapy from birth until adulthood which involves application of all available operative and conservative procedures for treatment (3). The osseous closure of the alveolar cleft, which is required for the formation of regular upper dental arch, occupies a special position with in the whole concept of cleft lip and palate therapy.
This case report presents the dental rehabilitation of adult female patient with unilateral cleft of lip, palate and alveolus with congenitally missing lateral incisor by multidisciplinary team approach.
CASE REPORT
Case history
A 17 year old female with unilateral cleft lip and palate was referred for dental rehabilitation. Her chief complain was unaesthetic appearance of her upper front teeth. She presented with unilateral cleft lip and palate of left side. She had received primary lip repair when she was 4 month old and palatoplasty when she was 2 years old respectively. She also had a history of lip revision at age of 4.
Clinical examination
The patient presented a mesoprosopic facial pattern orthognathic profile, slightly prominent chin with deviated nasal septum towards right side (Fig: 1). Intra oral examination revealed that she also had alveolar cleft. She had Angles Class I malocclusion with cross bite in relation to 13 & 43, 23 & 32 and 25 & 35(Fig: 2) .Lower mid line was shifted to left. The following teeth were missing - upper lateral incisor bilaterally, upper central incisor on left side and lower left canine. On smile bilateral buccal corridor space was visible.
Fig:1
Pre treatment extra oral photographs Fig:2
Pre treatment intra oral photographs Radiographic examination
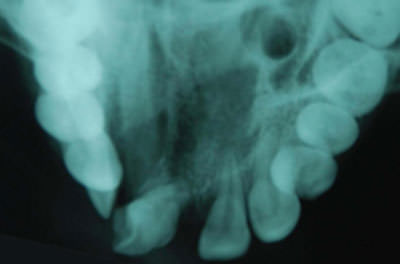
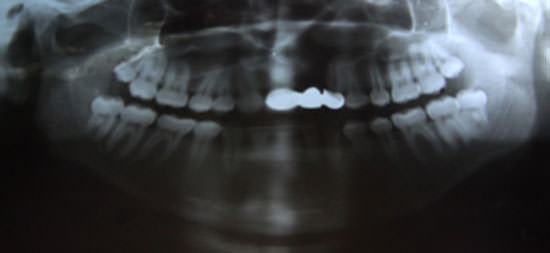
Panoramic, intra oral periapical and occlusal radiographs (Fig:3,4,5) confirmed the presence of alveolar cleft. Cephalometric evaluation( SNA-650,SNB-710,ANB -6 0 ,Wits- -7 mm) revealed class III skeletal pattern with proclined upper incisors ( 310, 7mm ) and severely retroclined lower incisors( 20,-1mm).She has average growth pattern and acute nasolabial angle (650)(Fig:6,Table:1)
Fig:3
Pre treatment OPG Fig:4
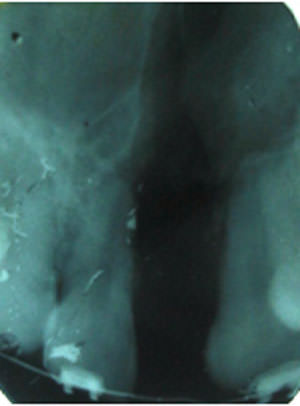
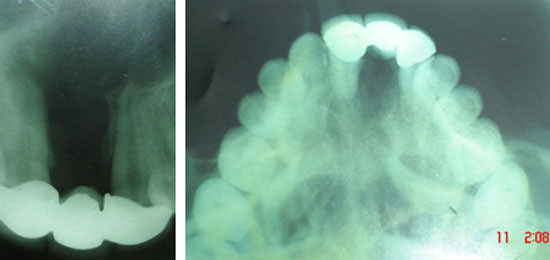
Pre treatment occlusal view Fig:5
Pre treatment IOPA Fig:6
Pre treatment lateral cephalogram Table:1
Cephalometric analysis Diagnosis
Skeletal class III pattern with Angle's Class I malocclusion with cross bite (in relation to 13 & 43, 23 & 32 and 25 & 35) and several missing teeth(12,21,22&33) with lower dental mid line shift towards left .She had alveolar cleft in between upper right central incisor and upper left canine with deviated nasal septum towards right side.
Treatment objectives
Maintenance of class I molar relation and positive overjet, Check on class III skeletal pattern, correction of smile, Correction of cross bite, correction of crowding, correction of lower midline shift, correction of alveolar cleft by bone graft and correction of nasal deformity.
Treatment plan
Treatment plan was formulated by consulting our interdisciplinary team which included Orthodontist, Endodontist, Oral and maxillofacial surgeon, Prosthodontist and Plastic surgeon. It was decided that once upper arch will be aligned with fixed orthodontic treatment, alveolar bone grafting will be done and then implant supported prosthesis for missing tooth will be given. Rhinoplasty will be done as final procedure to enhance the facial esthetics.
Orthodontic planning
Since patient had positive ovejet and only 10-25% of growth is remaining it was decided that non-surgical management with careful growth monitoring of class III skeletal pattern will be preferred. Two plans were thought for dental occlusal correction.
Replacement of missing upper right lateral incisor and upper left central incisor by prosthesis and finishing the case in class I occlusion. Upper left lateral will not be replaced in order to balance the Bolton's ratio since lower left canine was missing.
Extraction of lower right first premolar to correct the lower crowding and midline shift and replacement of upper left central incisor by prosthesis and reshaping of upper canines as lateral incisors and finishing the case in class I occlusion. Upper right &left laterals will not be replaced in order to balance the Bolton's ratio.
Selected treatment plan
Since the Cephalometric examination revealed that upper incisors were proclined and nasolabial angle was acute, we selected plan B ( i.e. extraction of lower right first premolar and replacement of upper left central incisor) in order to preserve soft tissue balance and to maintain incisor inclination . Plan A will require creation of space between upper right central incisor and right canine which will cause further increase in upper incisor proclination and worsening of nasolabial angle. There is chance of exposing the root of upper right central incisor to the alveolar cleft area.
Treatment progress
A Pre-adjusted .018 Roth appliance was bonded to maxillary arch and an .016 Niti round arch wire was placed for initial leveling and aligning. Upper anterior bite plane was given for vertical clearance for correction of cross bite. After initial alignment .016 x.022 rectangular Niti was placed. Lower arch bonding is delayed purposely to reduce the aggravation of cross bite. After 5 months of treatment lower right first premolar was extracted and lower arch bonding was done. Leveling and aligning of lower arch was done with the help of .016 and .016x.022 Niti wire in progression. After 8 months of treatment open coil spring on .016x .022 S.S wire was placed between upper right central incisor and upper left canine for creation of space for prosthesis for upper left central incisor. After adequate space is achieved alveolar bone grafting was done (Fig:7).
Fig:7
Post alveolar bone grafting IOPA
Once the lower arch leveling and aligning is achieved .016x .022 S.S wire was placed. Mild class III elastic was started at this stage to keep a check on mandibular growth. After 12 months of treatment remaining lower arch space was started to close with the help of closed vertical loop in .016x.022 S.S wire. At this stage patient was suggested for implant supported prosthesis for 21 in grafted area but patient has declined this option due to economical reason and hence it was decided that remaining upper space will be closed by fixed partial denture after finishing of orthodontic treatment. Coronoplasty of upper canines was done as upper lateral incisor. Finishing and detailing was done with upper and lower .016 Niti arch wire and box elastics. Case was debonded after 16 months of treatment. Upper Hawley's appliance with prosthesis for 21 is delivered as retainer. After 6 months of retention phase fixed partial denture was delivered. Treatment results were stable after 2 years of treatment. Later rhinoplasty was performed which has greatly improved the facial esthetics.
Treatment results
Post treatment record revealed that the treatment objectives are achieved .Facial photographs showed improved esthetics (Fig:8). Class I molar and class I canine relation was achieved. Midline was corrected. An acceptable overbite and over jet was achieved (Fig: 9).
Fig:8
Post treatment extra oral photographs Fig:9
Post treatment intra oral photographs
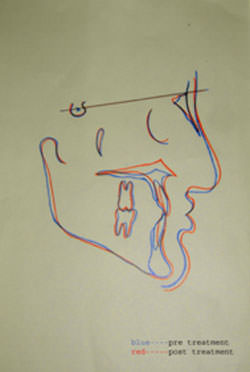
Post treatment lateral Cephalometric analysis and superimposition revealed slight skeletal change (ANB=10,wits=3mm Fig:10,11) .The maxillary and mandibular incisors were slightly retroclined (U1 to N-A =300,7mm,IMPA=740) in comparision with pre treatment (Table-1). A post treatment panoramic radiograph showed correction of root angulation of teeth adjacent to cleft area in comparison to pretreatment state (Fig: 12).
Fig:10
Post treatment cephalogram Fig:11
Cephalometric superimposition Fig:12
Post treatment OPG
Intra oral periapical radiographs and occlusal radiograph revealed that grafting of alveolar cleft was initially successful), but it resorbed ( Fig :13)over a period of two years in absence of functional stimulation.2 year post treatment record revealed that treatment results were stable (Fig:14,15)
Fig:13
2 years post treatment IOPA & Occlusal radiograph showing resorption of bone graft Fig:14
2 years Post treatment extra oral photographs Fig:15
2 years post retention intra oral photographs Discussion
The present case reinforces the need of multidisciplinary team approach for comprehensive management of cleft lip and palate patients. Ideally secondary alveolar bone grafting is done early around 9-11 years to allow eruption of canine into the grafted bone (Bergland et al 1986 (4) ,Brattstorm & McWilliam 1989 (5)).The other benefits of alveolar bone grafting is: to restore the function of maxillary arch at cleft site ,to provides bone support to the teeth adjacent to cleft site ( Waite and Kirsten 1980 (6)),it improves facial appearance through restoring facial symmetry ,provide alar base support and establishing nasolabial contour( Skoog ;1967 (7) Waite and Kirsten ;1980 (8) and Turvey ;1984 (8).) Several studies suggest that bone graft success decreases if performed after the eruption of permanent canine into the cleft site ( Turvey et al ;1984 (8), Bergland et al ;1986 (4) ).Patients with repaired cleft lip and palate often have a hypoplastic or absent maxillary incisor on the cleft side. The various option for replacement of missing lateral incisors are, closure of space with mesialization of the canine into lateral incisor position ,conventional removable prosthesis, fixed partial denture and implant supported prosthesis. The mesialization of canine at lateral incisor position and fixed partial denture may not be aesthetically acceptable if there is a defect of alveolar ridge (9) .Replacement of the lateral incisor with an osteointigrated implant provides better esthetics. The implant supported prosthesis in edentulous alveolar cleft is first reported by Verdi et al in 1991 (10). Kearns et al (11)(1997) shown that in his study that interval between bone graft and placement of an implant is important. The greater the interval beyond four months, the more likely it is that there will be inadequate bone volume to accept an implant. It has been shown that when alveolar cleft is covered by bridge, grafted bone undergoes a greater resorption due to missing functional stress 3. Similar resorption of bone graft is seen in this case. As literature supports that bone graft resorb if functional stimulus is not provided (3), it is of great importance that clinician should move adjacent teeth in to the grafted bone or motivate the patient for implant supported prosthesis in order to provide functional stimulus to the graft. Recontouring of different teeth by Endodontist or Prosthodontist enhance the patient smile.
Bibliography
Kim NY,Baek SH. Cleft sidedness and congenitally missing or malformed permanent maxillary lateral incisors in Korean patients with unilateral cleft lip and palate .Am J Orthod Dentofacial Orthop 2006;130:752-758 .
Suzuki A,Takahama Y. Maxillary Lateral incisors of subjects with cleft lip and/or palate :part 1. Cleft Palate Craniofacial J1992;29:376-379.
Demph R, Teltzrow T, Kramer FJ,Hausamen JE. Alveolar bone grafting in patients with complete cleft: A comparative study between secondary and tertiary bone grafting.Cleft Palate Craniofacial J.2002;39:18-25.
Bergland O,Semb G, Abyholm FE. Elimination of theresidual alveolar cleft by secondary bone grafting and subsequent orthodontic treatment. Cleft Palate Craniofacial 1986 ;.23:175-205 .
Brattstorm V,McWilliam J. The influence of bone grafting age on dental abnormalities and alveolar bone height in patients with unilateral cleft lip and palate. Europ J Orthod;1989:351-358.
Waite DE,Kersten RB.Residual alveolar and palatal clefts.In : Bell WH,Profitt WR,White RP,eds.Surgical correction of dentofacial deformities.Philadelphia:WB Saunders.1980,1329-1367.
Skoog T.The use of periosteoum and surgical for bone restoration incongenital clefts of the maxilla .Scand J Plast Surg.1967;1:113-130.
Turvey AT,Vig K,Moriarty J, Hoke J.Delayed bone grafting in cleft maxilla and palate: a retrospective multidisciplinary analysis. Am J Orthod 1984;86:241-256.
Stienberg B,Padwa BL, Boyne P, Kaban L .State of art in oral and maxillofacial surgery:Treatment of maxillary hypolplasia and anterior palatal and alveolar cleft. Cleft Palate Craniofacial J1999 ;36 :283-291 .
Verdi F,Lanzi G,Cohen S,Powell R.Use of Branemark implant in cleft palate patient. Cleft Palate Craniofacial J1991;28:301-303.
Kearns G,Perrott GH,Sharma A, Kaban LB,Vargervik K.Placement of endosseous implants in grafted alveolar clefts. Cleft Palate Craniofacial J 1997;34:520-525.