Introduction
Enhancing appearance and getting better psychological and social appraisal seems to play significant tasks in an individual's choice to begin orthodontic treatment.(1) Functional and aesthetic enhancements in occlusion are the common causes quoted by adults for taking orthodontic treatment.(2) Previous questionnaire studies are done among adults and established that, the key fascinating factor for taking orthodontic treatment was an aspiration to get better dental appearance, along with facial emergence.(3,4)
The uptake of orthodontic treatment has revealed to diverge distinctly in various populations, as of 5% to 60%, depending on the countryside.(5) The research on determining the factors that forecast undergoing of orthodontic treatment has spotlighted on young peoples and recognized various factors such as gender,(6) ethnic background,(7) socioeconomic status,(8) availability of orthodontic services,(8) and need of orthodontic treatment.(9)
The orthodontic treatment uptake is greater in females because of favoured self-selection and not essentially larger need.(7) The socioeconomic class is a noteworthy interpreter for orthodontic treatment.(8) The incidence of undergoing orthodontic treatment among younger people is greater in high as well as middle socioeconomic group but it is lesser in lower socioeconomic group.(8)
In the current system of oral health care, the spotlight is greater on (1) the capability to recognize the patients’ needs and individuals’ awareness of oral health importance, (2) the satisfaction of the patients’ with treatment, and finally (3) adults’ professed in general value of health systems.(10) There is an important role of OHRQOL, self-esteem and apparent need of orthodontic treatment in influencing treatment uptake. The adolescents taking orthodontic treatment were having 3.1 times additional poorer OHRQOL than the age-matched peers who were not undergoing orthodontic treatment.(11)
The aesthetic component (AC) of the index of orthodontic treatment need (IOTN) has been greatly used to promote for undergoing orthodontic treatment in matures with malocclusion.(12) In adolescents, the AC of IOTN was reported as a forecaster of orthodontic treatment.(9) The AC of IOTN has been assessed as an outcome of treatment in context to self-esteem. It has not been evaluated as a possible predictor for taking orthodontic treatment. Various studies have been done worldwide and evaluated factors such as gender,(6) ethnic background,(7) socioeconomic status,(8) availability of Orthodontic services,(8) orthodontic treatment requirements,(9) oral health related quality of life(13) and self-esteem(13) in predicting the taking of orthodontic treatment. After a thorough search of the literature databases in Pubmed, Scopus, Sciencedirect, Ebscohost, etc. till May, 2016, there was no study done in India to evaluate the OHRQOL, self-esteem, sociodemographic background and need of orthodontic treatment in prediction of orthodontic treatment uptake among adults.
Therefore the study aimed to evaluate and compare the function of orthodontic treatment need, socio-demographic background, self-esteem and OHRQOL, in predicting orthodontic treatment uptake among those who came to seek orthodontic treatment with age-matched adults.
Subjects and Methods
The study design was a cross-sectional study. The study was started after obtaining the ethical clearance from institutional ethics committee. The participants were selected based on the inclusion and exclusion criteria designed for the study. These participants were registered for the study after obtaining the written informed consent form. The participants were provided with a participant information sheet.
Sample description
The sample size was calculated from the previously done study by Johal et al.[13] The sample size was calculated with PS Power and Sample Size Calculations software PS Version 3.1.2, January 2009. The Statistical formula for calculation of sample size is as follows:
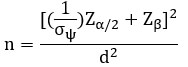
where, Zα/2= confidence level, Zβ= power, σψ= odds ratio, d= effect size and n= sample size.
2.5 and an effect size of 0.2. Therefore, the samples included in our study were 130 individuals who included 65 participants who had came to seek orthodontic treatment and 65 participants who were age-matched adults’ not seeking orthodontic treatment. The inclusion criteria were subjects aged 18 years and above and knowledge of English language. The exclusion criteria were subjects who were not ready to join in the study, loss of teeth because of caries or periodontal disease, previous orthodontic treatment and/ orthognathic surgery. The subjects who fulfilled the inclusion and exclusion criteria were registered for the study. From the participants registered for the study, those who came to seek orthodontic treatment were recruited in the experimental group and those who were not seeking orthodontic treatment were recruited in the control group. Therefore, the age-matched controls were those subjects who were fulfilling the inclusion and exclusion criteria of the study but they were not seeking orthodontic treatment irrespective of their malocclusion. Each participant was evaluated and the data related to socio-demographic background, need of orthodontic treatment, self-esteem and OHRQOL was collected.
Sociodemographic parameters consisted of gender, age, marital status, ethnic background, and socioeconomic status markers: education, employment status and occupation. Occupation is believed to be an indicator of social class. Education was assessed by the maximum qualification acquired, with elevated ranks representing postgraduate or university qualifications. The employment status information was divided into self-employed or being an employee. Regarding marital status the subjects were divided into without a partner or with a partner.
The need of orthodontic treatment was evaluated using the index of orthodontic treatment need (IOTN). Each participant’s dental health was measured with the dental health component of IOTN. It was measured by the principal investigator after a thorough clinical examination according to the format of DHC of IOTN and the participants were categorized into no need, little need, borderline and definite need of orthodontic treatment. Each participant’s self-perceived dental aesthetics was evaluated with the aesthetic component of IOTN. Pictorial scale of ten colour pictures presenting different levels of dental attractiveness was given to the participant. The participants were provided with a mirror and were asked to match their dentition within that 10 colour photographs which best fits their dentition. Then according to it, the participants were categorized by the principal investigator into no need, borderline and definite need of orthodontic treatment.
questionnaires were collected from the participants. The RSES consists of ten questions out of which 5 are positive and 5 are negative. The answers for the positive and negative items were weighed separately on a 4-point Likert scale, counting strongly agree (SA), agree (A), disagree (D), and strongly disagree (SD). Positive questions are measured as 3=Strongly Agree, 2=Agree, 1=Disagree and 0=Strongly Disagree. Reverse scoring is done in negative questions that is, 0=Strongly Agree, 1=Agree, 2=Disagree and 3=Strongly Disagree. The sum of the scores for all the 10 questions was calculated. The total scale of the score varies from 0 to 30. The higher the score, higher is the self esteem.
The OHIP-14 questionnaire was utilized to assess the oral health impact on quality of life. The printed OHIP-14 questionnaire was provided to the participants. Filled questionnaires were collected from the participants and evaluated. The OHIP-14 has seven perception domains (two questions per domain) thus 14 questions. The domains are physical disability, functional limitation, social disability, psychological discomfort, physical pain, handicap and psychological disability. The answer to each question was measured with a five-point Likert scale where never is scored as 0; hardly ever as 1; occasionally as 2; fairly often as 3; and very often or every day as 4. The sum of the scores for all the 14 questions was calculated. The total scale of the score ranges from 0 to 56. The higher the score of OHIP-14 greater is the negative impact on OHRQOL.
Results
In total, 130 adults were recruited for the study. There were equal numbers of test and control subjects. All subjects were between the age group of 18-56 years. The mean age of the sample was 30.83±11.75 years (Table 1).

Table 1: Age group (years)
In previous studies the reported mean ages of their samples were 40 years (13), 34 years (16) and 25 years (3) respectively. Additionally these studies had divided their sample into two groups based on the mean age of their sample to predict the factor related to uptake of orthodontic treatment. Since the mean age of our sample was 30.8 years, the sample was divided into less than and greater than 30 years of age.
There was a large and statistically significant difference (P<0.0001) in taking orthodontic treatment between age group less than 30 years (85.91%) and more than 30 years (6.78%) (Table 2). The increased number of subjects undergoing orthodontic treatment were less than 30 years old (OR=83.9; 95% CI=24.87-282.81; Table 2).
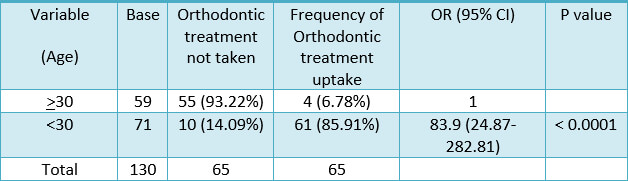
Table 2. Frequency of age, odds ratio, and 95% confidence interval to predict orthodontic treatment uptake with simple logistic regression analyses (N=130)
There was a statistically significant difference in taking orthodontic treatment amongst males and females (P=0.0364; Table 3). Females are more choosing orthodontic treatment (OR=2.11; 95% CI=1.04-4.25; Table 3).
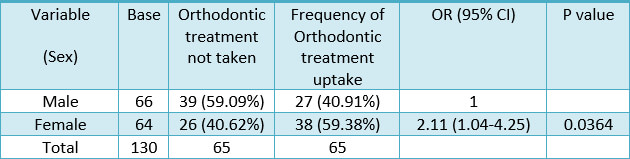
Table 3. Frequency of sex, odds ratio, and 95% confidence interval to predict orthodontic treatment uptake with simple logistic regression analyses (N=130)
There was a large and statistically significant difference (P<0.0001) in taking orthodontic treatment among subjects without a partner (66.67%) and subjects with a partner (19.57%). The increased number of subjects undergoing orthodontic treatment were without a partner (OR=8.22; 95% CI=3.48-19.39; Table 4).
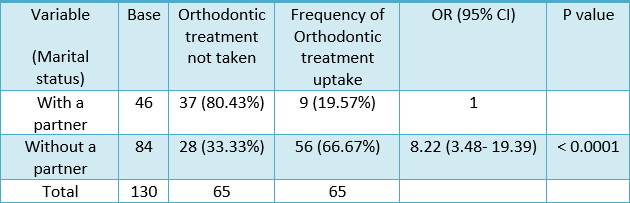
Table 4. Frequency of marital status, odds ratio, and 95% confidence interval to predict orthodontic treatment uptake with simple logistic regression analyses (N=130)
The difference in taking orthodontic treatment between individuals with high social class (50.62%) and those with low social class (48.98%) was not statistically significant (P=0.8564; OR=0.93; 95% CI=0.46-1.90; Table 5).
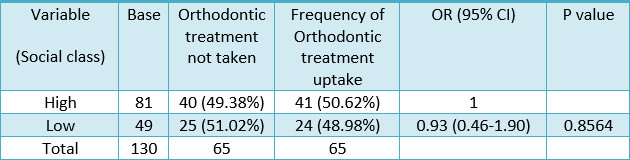
Table 5. Frequency of social class, odds ratio, and 95% confidence interval to predict orthodontic treatment uptake with simple logistic regression analyses (N=130)
The difference in taking orthodontic treatment between individuals with high education (52.94%) and those with low education (39.29%) was not statistically significant (P=0.2034; OR=0.57; 95% CI=0.24-1.34; Table 6).
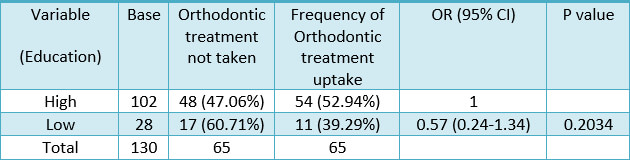
Table 6. Frequency of education, odds ratio, and 95% confidence interval to predict orthodontic treatment uptake with simple logistic regression analyses (N=130)
There was a large and statistically significant difference (P=0.7250; Table 7) in taking orthodontic treatment between employee (51.43%) and self-employed (48.33%) subjects. The increased number of subjects undergoing orthodontic treatment were employee (OR=1.13; 95% CI=0.56-2.25; Table 7).
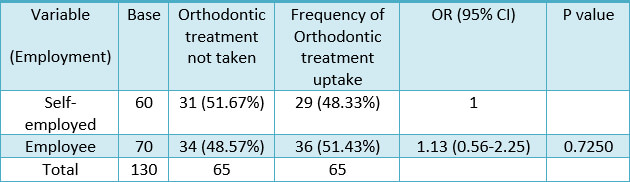
Table 7. Frequency of employment, odds ratio, and 95% confidence interval to predict orthodontic treatment uptake with simple logistic regression analyses (N=130)
There was a statistically significant difference (P=0.5873; Table 8) in taking orthodontic treatment among subjects with low need or great need (as measured by the clinician using the DHC of the IOTN). The increased number of subjects undergoing orthodontic treatment were those with a great need (OR=1.21; 95% CI=0.59-2.47; Table 8).
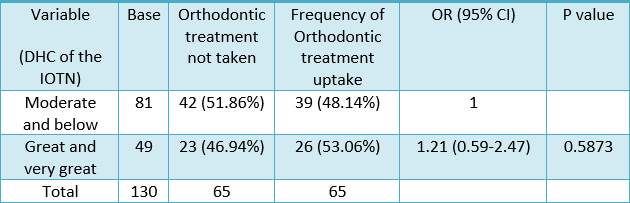
Table 8. Frequency of need for orthodontic treatment (DHC of the IOTN), odds ratio, and 95% confidence interval to predict orthodontic treatment uptake with simple logistic regression analyses (N=130)
The difference in taking orthodontic treatment between individuals with a need and without a need (as measured by the subject using the AC of the IOTN) was not statistically significant (P=0.8552; OR=0.93; 95% CI=0.45-1.91; Table 9).
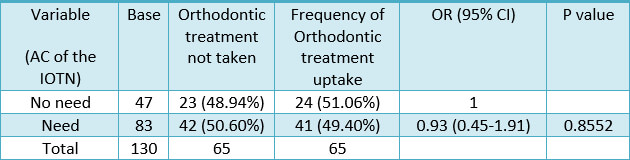
Table 9. Frequency of need for orthodontic treatment (AC of the IOTN), odds ratio, and 95% confidence interval to predict orthodontic treatment uptake with simple logistic regression analyses (N=130)
The OHIP-14 score ranged from 3-56 with a mean of 36.43±14.62 (Table 10). In relation to OHRQOL, there was a large and statistically significant difference (P=0.1129; Table 11) in taking orthodontic treatment among subjects with high impact of oral health (56.16%) and low impact of oral health (42.10%). The increased number of subjects undergoing orthodontic treatment were those with high impact of oral health (OR=1.76; 95% CI=0.87-3.54; Table 11).

Table 10. OHRQOL (OHIP-14 score)
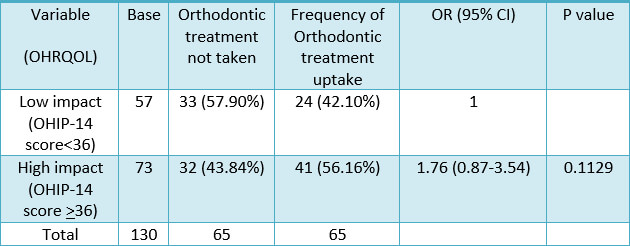
Table 11. Frequency of OHRQOL, odds ratio, and 95% confidence interval to predict orthodontic treatment uptake with simple logistic regression analyses (N=130)
The RSES score ranged from 2-30 with a mean of 20.06±7.02 (Table 12). With regard to Self-esteem, there was a large and statistically significant difference (P=0.7257; Table 13) in taking orthodontic treatment between subjects with an elevated self-esteem (51.52%) and with a low self-esteem (48.43%). The increased number of subjects undergoing orthodontic treatment were those with a high self-esteem (OR=1.13; 95% CI=0.56-2.25; Table 13).

Table 12. Self-esteem (RSES score)
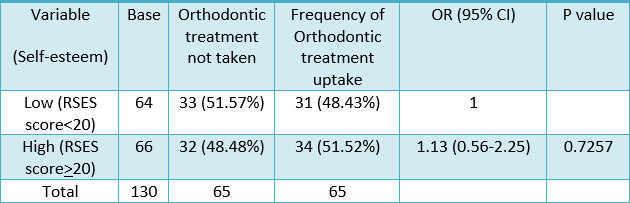
Table 13. Frequency of self-esteem, odds ratio, and 95% confidence interval to predict orthodontic treatment uptake with simple logistic regression analyses (N=130)
A multiple logistic regression analysis was used to confirm the importance of the recognized predictors of orthodontic treatment uptake and show their collective effects. The covariates that were entered into the regression model were age, sex, marital status, employment, DHC of IOTN, OHRQOL and self-esteem. The regression model confirmed the significance of age, sex, marital status, employment, OHRQOL and self-esteem (Table 14).
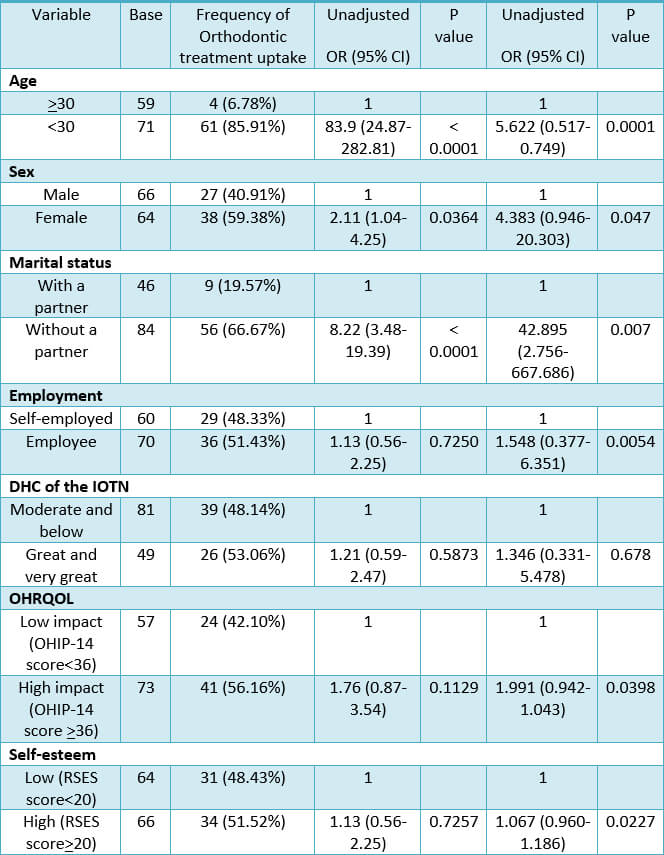
Table 14. Frequency distribution, unadjusted odds ratios, adjusted odds ratios, and 95% confidence intervals to predict orthodontic treatment uptake with a multiple logistic regression analysis (N=130)
Discussion
This is the first cross-sectional study done in India which assessed the factors that forecast taking of orthodontic treatment among adults in India. This type of research is carried out because in clinical practices it is observed that there is an increase in adult patients.(14,15) The adults are increasing for taking orthodontic treatment because of consciousness of their facial appearance, communal acceptance of treatment, advanced manifestation of appliances, and rising disappointment with earlier treatment interferences.(3) Therefore we should understand the factors that forecast the taking of orthodontic treatment and it should be added to the informed consent form thereby improving the satisfaction of the patient with treatment.
Earlier studies have demonstrated that females are more unsatisfied with the look of their teeth and demand a need for treatment more frequently than do males.(2,7) In one study it was found that increased number of adults taking orthodontic treatment were less than 40 years of age.(2) This is similar to the results of other studies with accounted mean ages of 34 and 25 years.(16,3) In relation to marital status, there was a large and statistically significant variation in taking orthodontic treatment among subjects without a partner and with a partner. For those who are adolescent and single, their physical appearance plays a key role in community relations. From childhood to maturity, good-looking individuals are treated specially and seen further optimistically and socially skilled. They are readily chosen as friends and are more successful in their occupation.(17,18) The key motivating factor for adults taking orthodontic treatment was a wish to straighten the teeth and get better smile.(16)
In relation to need of orthodontic treatment, the variation in taking orthodontic treatment among individuals with a need and without a need (as measured by the subject using the AC of the IOTN) was not statistically significant. Many individuals taking orthodontic treatment were not conscious of their malocclusion, as shown by their scores of the aesthetic component of the IOTN, which states that there was some aesthetic impairment.(11) The results of this study disagrees with other results that have found poor perceptions of teeth and increased dental consciousness among adults with malocclusion.(12) Adding weight to it, other studies have spotlighted on assessing the intention of adults taking orthodontic treatment.(3,16) When adolescents taking orthodontic treatment were evaluated by clinician and patients, it was found that those who were taking orthodontic treatment were having severe malocclusions and better visual impacts.(9,11)
The uptake of orthodontic treatment in adults is influenced by self-esteem. But other studies have accounted that there is no association of dentofacial deformity with low self-esteem.(19,20) But from the results of our study, self-esteem is associated with the perceived need for orthodontic treatment; hence, it is related to the uptake of orthodontic treatment.
In relation to OHRQOL, there was a large and statistically significant variation in taking orthodontic treatment among subjects with high and low impact of oral health. In other study, similar results were accounted in which adolescents taking orthodontic treatment were judged and it was found that those who had taken treatment were having negative impact of OHRQOL.(11)
The multiple logistic regression analysis confirmed the significance of age, sex, marital status, employment, OHRQOL and self-esteem in predicting the uptake of orthodontic treatment.
Conclusion
The importance of age, sex, marital status, employment, OHIP-14 and the Rosenberg self-esteem scale (RSES) in forecasting the uptake of orthodontic treatment among matures was recognized.
Referencias bibliográficas
- Byrne D, London O, Reeves K. The effects of physical attractiveness, sex, and attitude similarity on interpersonal attraction. J Pers 1968; 36:259-71.
- Cunningham S, Hunt N, Feinmann C. Psychological aspects of orthognathic surgery: a review of literature. Int J Adult Orthod Orthognath Surg 1995; 10:159-64.
- McKiernan E, McKiernan F, Jones M. Psychological profiles and motives of adults seeking orthodontic treatment. Int J Adult Orthod Orthognath Surg 1992; 7:187-98.
- Sergl HG, Zentner A. A study of psychological aspects of adult orthodontic treatment. Int J Adult Orthognath Surg 1997; 12:17-22.
- Foster Page LA, Thomson WM. Malocclusion and uptake of orthodontic treatment in Taranaki 12-13-year-olds. N Z Dent J 2005; 101:98-105.
- Kerosuo H, Abdulkarim E, Kerosuo E. Subjective need and orthodontic treatment experience in a Middle East country providing free orthodontic services: a questionnaire survey. Angle Orthod 2002; 72:565-70.
- Harris EF, Glassell BE. Sex differences in the uptake of orthodontic services among adolescents in the United States. Am J Orthod Dentofacial Orthop 2011; 140:543-9.
- Badran SA, Al Khateen S. Factors influencing the uptake of orthodontic treatment. J Public Health Dent 2013; 73:339-44.
- Mandall NA, Wright J, Conboy F, Kay E, Harvey L, O’Brien KD. Index of orthodontic treatment need as a predictor of orthodontic treatment uptake. Am J Orthod Dentofacial Orthop 2005; 128: 703-7.
- De Oliveira C, Sheiham A. Orthodontic treatment and its impact on oral health-related quality of life in Brazilian adolescents. J Orthod 2004; 31:20-7.
- Feu D, de Oliveira BH, de Oliveira Almeida MA, Kiyak HA, Miguel JA. Oral health related quality of life and orthodontic treatment seeking. Am J Orthod Dentofacial Orthop 2010; 138:152-9.
- Helm S, Kreiborg S, Solow B. Psychosocial implications of malocclusion: a 15-year follow-up study in 30-year-old Danes. Am J Orthod 1985; 87:110-8.
- Johal A, Joury E. What factors predict the uptake of orthodontic treatment among adults? Am J Orthod Dentofacial Orthop 2015; 147:704-10.
- Khan R, Horrocks E. A study of adult orthodontic patients and their treatment. Br J Orthod 1991;18:183-94.
- Nattrass C, Sandy J. Adult orthodontics-a review. Br J Orthod 1995;22:331-7.
- Pabari S, Moles D, Cunningham S. Assessment of motivation and psychological characteristics of adult orthodontic patients. Am J Orthod Dentofacial Orthop 2011;140:e263-72.
- Baldwin D. Appearance and aesthetics in oral health. Community Dent Oral Epidemiol 1980;8:244-56.
- Jacobsen A. Psychological aspects of dentofacial esthetics and orthognathic surgery. Angle Orthod 1984;54:18-35.
- O’Regan J, Dewey M, Slade P, Lovious B. Self-esteem and aesthetics. Br J Orthod 1991;18:111-8.
- Varela M, Garcia-Camba J. Impact of orthodontics on the psychologic profile of adult patients: a prospective study. Am J Orthod Dentofacial Orthod 1995;108:142-8.