Introduction
With the soft tissue paradigm shift, several factors are being considered during the initial diagnosis of an orthodontic case. The facial aesthetics are taking priority over the ideal dental norms. This helps to evaluate the final treatment plan and to address the issue of requirement of extraction of teeth. In 1998, Dr.Castanon et.al developed the Churro jumper (1). This fixed functional appliance was easy to fabricate and was to be an economical solution to the more expensive alternatives on the market.
Diagnosis
A 15 year old male patient reported to the clinic with the chief complaint of proclined upper teeth. He was diagnosed as having class 2 div.1 malocclusion with proclined maxillary anterior teeth with visible spacing and also a retrognathic mandible.
Extra Oral Photographs

Fig.1: Extra Oral- Frontal, Fig.2: Extra Oral frontal –Smile, Fig.3: Extra oral – Profile, Fig.4: Extra Oral Three quarter
Intra Oral Photographs

Fig.5 Intraoral Frontal, Fig.6: Intraoral Left Buccal view

Fif.7 Intraoral Maxillary Occlusal, Fig.8 Intraoral Mandibular Occlusal

Fig.9 Pretreatment profile view, Fig.10 Visual Treatment Objective : Positive
As the visual treatment objective was noted to be positive, mandibular repositioning was decided to be the best course of action with a non extraction treatment plan. An MBT prescription metal bracket system with an .022” bracket slot was used. The initial leveling and aligning was completed using the light gauge wires, followed by rectangular NiTi archwires and Rectangular stainless-steel arch wires.
After the teeth were judged to have attained the proper tip and torque, the jasper jumper appliance was placed(2).

Fig.11: Jasper Jumper Intra Oral Frontal View Fig.12: Jasper Jumper buccal view
In about 2 months of placement of the jasper jumper appliance the patient had arrived at the clinic with a broken appliance and did not prefer to have it replaced. We were on the lookout for a more economical solution. The Churo Jumper seemed to be a logical substitutedue to its ease of fabrication and because it the suited the patient’s affordability. Therefore, the Churo Jumper was selected as a substitute to the jasper Jumper.
Construction of the Churo Jumper
The linear measurement was performed between the distal aspect of the mandibular canine and the mesial aspect of the maxillary first molar, the 10 mm was added to this length and was considered to the required length of the appliance (1). A wire of.028” was used to fabricate this appliance. About 15 coils were fabricated and placed between the maxillary first molar and the mandibular canine. A polyvinyl impression material was injected into the lumen of the coils with the help of a syringe. This step is performed in order to prevent pinching of the cheeks by the appliance.
The distal ends of the pain arch wire are cinched distal to the molar brackets. The appliance is placed after the leveling and aligning phase is completed.

Fig.1 3 Churo Jumper – Intraoral frontal view, Fig.14 Churo jumper – Intra oral Bucaal view left, Fig.15 Churo Jumper – Intra oral Buccal view right
Post Treatment Photographs

Fig.16. Post treatment extra oral, Fig.17 Post treatment extra oral smiling, Fig.18 Post treatment extra oral profile, Fig.19 Post treatment extra oral three quarter
Intra Oral Photographs

Fig.20 Post treatment Intra oral buccal view right, Fig.21 Post treatment Intra oral Frontal, Fig.22 Post treatment Intra oral buccal view left

Fig.23 Post treatment Intra oral maxillary occlusal View, Fig.24 Post treatment Intra oral mandibular occlusal View
Results
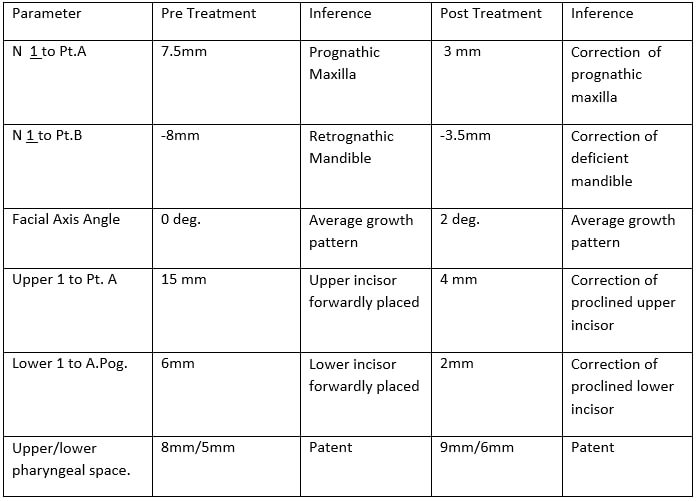
The proclined upper anterior teeth were corrected. The mandible was repositioned and the final post treatment profile was favorable. We were able to achieve competency of lips. The final dental position was determined to be a favorable class I malocclusion. The anchor loss was negligible.
Table 1
Discussion
According to a research done by Bjork.et.al, any increase in the vertical facial height for a Class II malocclusion patient would prove detrimental to the patient as the mandible rotates posteriorly and this causes worsening of the Class II pattern3. Therefore, if any orthodontic appliance was to cause a counter clockwise rotation of the mandible, it would help with the correction of the Class II malocclusion and prevent it from worsening.
This is the basis of correction of the Class II malocclusion with the help of functional appliances (fixed or removable ).
When the patient arrived to the clinic with the pre existing Class II malocclusion and incompetent lips several treatment plans were considered. Considering the patient’s age and a positive Visual Treatment Objective (VTO), a non extraction treatment plan was proposed with the help of a fixed functional appliance.
Several appliances were considered such as the Forsus appliance4, the Eureka spring5 and finally a decision was taken to use the Jasper Jumper appliance. During the initial assessment period, it was noted that the appliance was producing favorable results. After the patient broke the appliance, he was advised for replacement of the appliance but he found the solution expensive.
After a lot of contemplation, it was decided to use the Churo jumper as a favorable and economic replacement for the broken Jasper Jumper. The Churo jumper was placed and the final results were self evident. The class II malocclusion was corrected and the patient was able to attain a class I malocclusion and a favorable profile.
Conclusion
Although the fixed functional appliance therapy is effective and overcomes the shortcomings of patient compliance in traditional myofunctional therapy, they have certain limitations/. The constant breakages and difficulty in patient acceptance are some of the problems faced by the orthodontic practitioner. The Churo jumper is an economic and reliable substitute for the more expensive fixed functional appliances in the market.
References
- Ricardo C. et.al. Clinical sue of Churo jumper – J clin Orthod.1998;32:731-745
- Jasper J. Mc Namra JA. Correction of inter arch malocclusions using a fixed force module . Am J Orthod. 1995; 108: 641-50
- Bjork A. Prediction of mandibular growth rotation . Am J Orthod. 1969;55 (6):39-53
- Vogt W. The Forsus Fatigue resistant device. J clin Orthod 2006 : 368-77
- Devincenzo J. The Eureka Spring : A new internal force delivery system. C clin Orthod 1997: 45467