INTRODUCTION
Malocclusion, particularly when associated with crowding, can negatively impact an individual's social interactions, as facial aesthetics play a crucial role in how society perceives attractiveness, as well as in shaping one’s self-image. Dental crowding typically arises when there is a descrepancy between tooth size and the available arch space(1). Treatment decisions for crowding are influenced by several factors, including the severity of the crowding, the patient’s age, facial structure, and the specific type of malocclusion present(2).
Studies have shown that crowding is most prevalent in the anterior region and decreases progressively towards the posterior region(3). Since the anterior teeth are the most visible during smiling, their proper alignment is essential for achieving desirable aesthetics in orthodontic treatment(4). The main goal in managing severe crowding is to restore facial balance with a harmonious soft tissue profile, ensure proper occlusal function, and achieve an attractive smile(5).
Among dental anomalies, rotation is notably common, accounting for 10.24% of cases in the Indian population. The most commonly affected teeth are the mandibular second premolars (2.14%), followed by the mandibular first premolars (1.69%) and the maxillary central incisors (1.60%).Rotations were found to be more prevalent in females, particularly in the mandibular second premolars and maxillary central incisors(6). Typically, these rotations range between 45° to 90°, occurring mesiolingually along the tooth's long axis(7).
In untreated individuals, the prevalence of rotated teeth is estimated between 2.1% and 5.1%.Class I malocclusion can be managed through comprehensive orthodontic treatment using one of two primary approaches: extraction or non-extraction(8). The present case illustrates the successful management of severe maxillary crowding in a Class I malocclusion through a non-extraction treatment strategy.
CASE REPORT
A 13-year-old female student was referred to the Department of Orthodontics and Dentofacial Orthopedics,MINDS,with the chief complaint of irregularly placed upper and lower front teeth.The patient had no relevant medical history. Temporomandibular joint (TMJ) examination showed no history of pain and clicking while engaged in various jaw movements.In the extraoral examination, frontal and profile soft tissue revealed a symmetrical and balanced facial pattern with a convex profile and competent lip at rest (Figure 1).
Intraoral examination revealed a Class I molar relation on both sides with maxillary and mandibular crowding.Upper arch was U shaped with anterior spacing,Distopalatally rotated 21,Mesiobuccally rotated 11 and 25,Erupting 12,13,14 and 15.Lower arch was U shaped with lower anterior crowding and lingually placed 42.Anterior crossbite in relation to 11,12 and 21 were present.(Figure 2)
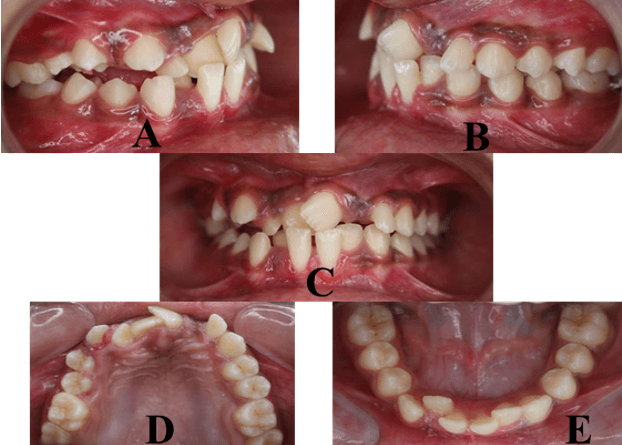
Figure 2:Intraoral examnation,A.Right lateral,B.Left lateral,C.Frontal,D.Maxillary arch,E.Mandibular arch
Radiographic examination confirmed severe rotation of left maxillary central incisor and revealed that 3/4 root of all teeth was completed.Deciduous tooth 62 which was extracted prior to the orthodontic treatment.Tooth buds of 18,28,38 and 48 was present. The lateral cephalometric analysis revealed a skeletal Class I with orthognathic maxilla and mandible and horizontal growth pattern and mandibular plane were normal.(Figure 3)
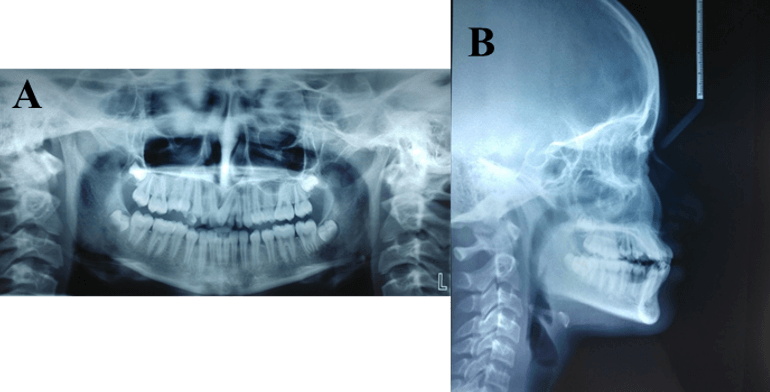
Figure 3:Radiographic examination,A.OPG,B.Lateral cephalogram
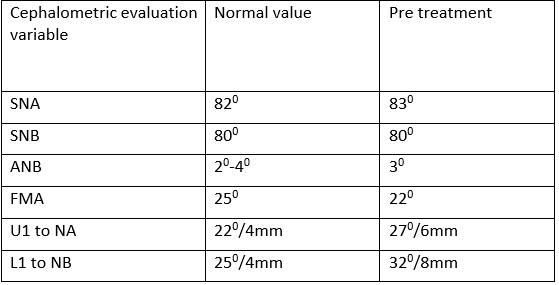
Cephalometric values show that upper and lower incisors were proclined (Table 1).After taking an alginate impression to fabricate study model,space analysis on study models did not show any space deficiency.
Table 1:Pretreatment cephalometric values
Based on the information gathered from the clinical examination and the diagnostic records, the treatment plan included relieving the maxillary and mandibular crowding using a maxillary and mandibular fixed appliance with non-extraction pattern. After appropriately prophylactically cleaning the labial and lingual surfaces of all teeth bonding was done in the upper arch using 0.022 slot Preadjusted edgewise brackets,MBT prescription.Banding was done on upper first permanent molars and lingual tube were soldered on the palatal side of bands. A removable posterior bite plane was given in the lower arch to relieve anterior crossbite.Modified Transpalatal arch with a hook on the left side extending to the palatal surface of left maxillary permanent second premolar was fabricated and attached to the lingual tube of maxillary permanent first molars.Lingual button was bonded to the labial surface of left maxillary central incisor and an e-chain was placed from modified transpalatal hook to lingual button to correct overlapping of 21 .0.012 NiTi archwire was placed on all upper teeth except 21(Figure 4).
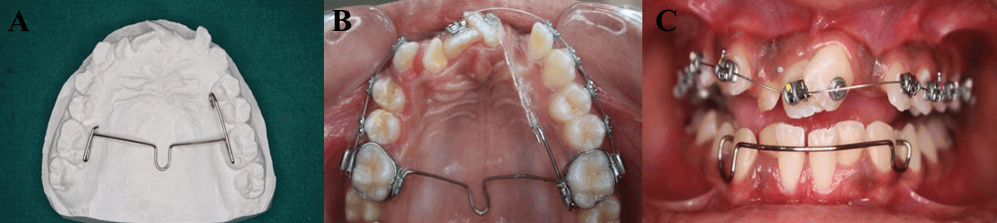
Figure 4:A.Fabricated modified TPA,B.Placement of modified TPA,C.Removable posterior bite plane.
After 6 weeks,overlap correction was achieved ,21 was bonded and continuous archwire is engaged on all teeth.Lower teeth also bonded using 0.022 slot preadjusted edgewise brackets,MBT prescription and lower molars were banded (Figure 5).Alignment and leveling procedures were followed by installing 0.14,0.016,0.018,0.017x0.025,0.019x0.025 NiTi archwires and were completed using 0.019x0.025 SS archwire.
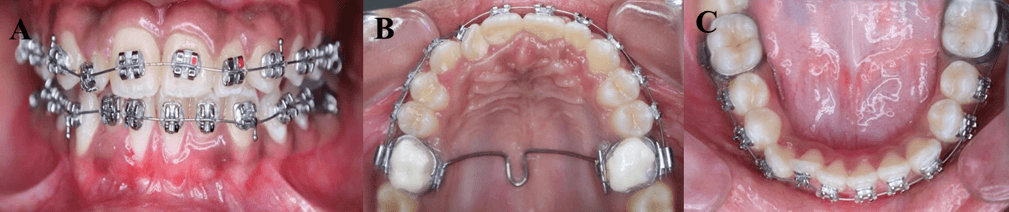
Figure 5:A,B.Intraoral photographs after correction of rotation,C.Mandibular arch
Finishing was done using 0.14 SS archwire. At the end of treatment removable retainer appliance was fabricated and given to the patient for one year to maintain the corrected tooth position.Six months of follow up showed no signs of relapse.(Figure 6,7)
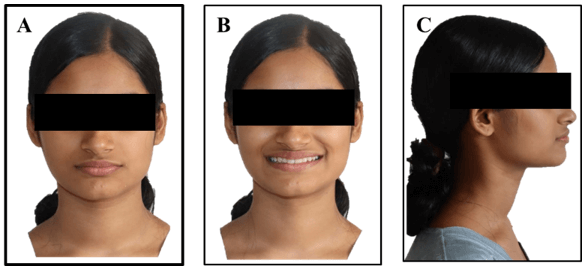
Figure 6: Post treatment extraoral photographs,A.Frontal,B.Smile,C.Profile
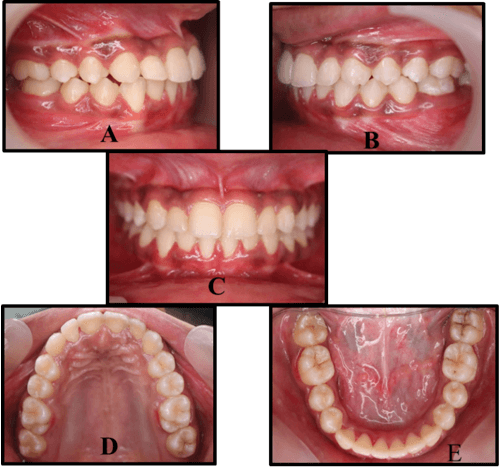
Figure 7: Post treatment intraoral photographs,A.Right lateral,B.Left lateral,C.Frontal,D.Maxillary arch,E.Mandibular arch
DISCUSSION
Orthodontists must evaluate different treatment options based on the patient’s skeletal and dental characteristics. Tooth rotation refers to the visible mesiolingual or distolingual displacement of a tooth within its alveolar socket along its long axis. Crowding can arise from genetic predisposition, environmental influences, or more frequently, a combination of both. Clinical assessment and patient history often reveal that malocclusion stems from dental factors(8). While genetic factors primarily determine tooth size, both hereditary and environmental influences affect dental arch shape and width(9).
For Class I malocclusion with crowding, orthodontic treatment may involve extraction or non-extraction methods such as interproximal reduction, dental arch expansion or molar distalization. The treatment choice typically depends on the severity of crowding and the patient’s facial profile(10). Cobourne et al. suggested that moderate crowding (5–8 mm) may require first or second premolar extractions, whereas severe crowding (>8 mm) often necessitates first premolar extraction(11).
In the presented case, space analysis indicated no significant arch length deficiency, leading to a non-extraction approach for crowding correction. Traditional treatment for rotated teeth involves fixed appliances, which anchor to select teeth rather than the entire permanent dentition. Although archwire elongation allows for greater torque with lighter forces, it also increases the risk of wire breakage, distortion, or displacement. A drawback of fixed appliances is compromised oral hygiene, which may cause decalcification around banded or bonded teeth(12).
For mixed dentition, a whip appliance can address rotations(13). Alternatively, a removable appliance with a labial bow and palatal spring (e.g.-Z-spring) can generate the necessary force to derotate teeth(14). However, this method is limited to maxillary central incisors and cannot correct severe or multiple rotations(15). While rotations are relatively straight forward to correct, retention remains challenging due to the slow adaptation of supra-alveolar and transseptal gingival fibers. Overcorrection and prolonged retention are often necessary to ensure long-term stability and prevent relapse(16).
CONCLUSION
Following active treatment, an optimal facial profile and functional occlusion were attained. The treatment duration of 17 months effectively resolved maxillary and mandibular crowding while significantly enhancing occlusal alignment, dental aesthetics, and facial harmony. All of the patient’s initial concerns were addressed, resulting in a more balanced smile and improved facial profile.
REFERENCES
- Pramustika A, Widayati R. Treatment of a Class I Malocclusion with Severe Crowding using Passive Self-Ligating Brackets. Journal of Dentistry Indonesia. 2020;27(2):109-13.
- Rahbar MI, Chaudhry NA. DENTAL CROWDING AND ITS RELATIONSHIP TO ARCH DIMENSIONS--GENDER DIMORPHISM. Pakistan Oral & Dental Journal. 2010 Dec 1;30(2).
- Hassan R, Rahimah AK. Occlusion, malocclusion and method of measurements-an overview. Archives of orofacial sciences. 2007;2:3-9.
- Shigenobu N, Hisano M, Shima S, Matsubara N, Soma K. Patterns of dental crowding in the lower arch and contributing factors: a statistical study. The Angle Orthodontist. 2007 Mar 1;77(2):303-10.
- Ahmed N, Younus A A, Joseph R, Bhat KRR, Nikhil P M, Haritha U. Treatment of severe crowding with constricted arches in a patient with high angle Class I malocclusion: A case report. Int J Oral Health Dent 2022;8(2):194-197.
- Gupta SK, Saxena P, Jain S, Jain D. Prevalence and distribution of selected developmental dental anomalies in an Indian population. Journal of oral science. 2011;53(2):231-8.
- Parisay I, Boskabady M, Abdollahi M, Sufiani M. Treatment of severe rotations of maxillary central incisors with whip appliance: Report of three cases. Dental Research Journal. 2014 Jan;11(1):133.
- Al-Refeidi E, Gammash M, Mohammed SH, Syed S, Togoo RA. Crowding, Spacing and closed dentition in Primary Dentition and its relationship with BMI among Saudi Children. Scholars Journal of Dental Sciences. 2016;3(12):312-6.
- Giri J, Bockmann M, Brook A, Gurr A, Palmer L, Hughes T. Genetic and environmental contributions to the development of dental arch traits: a longitudinal twin study. European Journal of Orthodontics. 2025 Apr;47(2):cjaf018.
- Al-Ani MH, Mageet AO. Extraction Planning in Orthodontics. The journal of contemporary dental practice. 2018 May 1;19(5):619-23.
- Cobourne MT, DiBiase AT. The orthodontic patient: Treatment planing. In: Handbook of orthodontics. 1st ed. Philadelphia: Elsevier; 2010:182-202.
- Hess E, Campbell PM, Honeyman AL, Buschang PH. Determinants of enamel decalcification during simulated orthodontic treatment. The Angle Orthodontist. 2011 Sep 1;81(5):836-42.
- Thakur S. International journal of scientific research. children. 1981;3(2):204-15.
- Correction of a severely rotated maxillary central incisor with the Whip device Arezoo Jahanbin a,*, Bahareh Baghaii b, Iman Parisay
- Verma J, Ahuja V. Alignment of rotated permanent maxillary central incisors with segmental orthodontics in mixed dentition: A case report. J Dent Panacea 2021;3(4):185-189.
- Ahrens DG, Shapira Y, Kuftinec MM. An approach to rotational relapse. American Journal of Orthodontics. 1981 Jul 1;80(1):83-91.